Modern understanding of obesity has changed, as medical professionals now recognize that obesity is not simply a result of a lack of willpower; rather, it’s a chronic disease. That shift is making the new class of anti-obesity drugs like Wegovy especially valuable. These drugs are highly effective, well-tolerated and safe, and they could improve the health and lives of millions. But these medications are very expensive, and paying for them will represent an enormous challenge to employer-sponsored health insurance. In the following article, we review the promise of this new class of medications, and various potential employer approaches to addressing the attendant high costs.
Obesity: Assessing the problem
Obesity rates have increased dramatically over recent decades; 42% of the U.S. adult population is now obese, and 31% is overweight. Obesity is associated with poor medical outcomes, including higher rates of type 2 diabetes, heart disease, degenerative arthritis, depression and many cancers. Those who are obese also face social discrimination and are likely to be underpaid and promoted less frequently. Obesity is also a health equity issue; those who have lower income and people of color are more likely to be obese.
Losing weight is difficult, especially for the obese. Our bodies have evolved to maintain weight by slowing metabolism when we eat fewer calories. Even highly motivated people who were able to lose huge amounts of weight through programs like “Biggest Loser” have struggled to maintain that weight loss.
Many efforts to combat obesity have failed to help, and some were dangerous. Most dietary interventions lead to short-term weight loss, but people regain weight rapidly. Some weight loss companies trumpet misleading success rates by selectively reporting results for a minority of participants. Previously available anti-obesity drugs were often only moderately effective, and often had bad side effects. One combination drug, fenfluramine/phentermine, was taken off the market when it was found to cause life-threatening pulmonary hypertension and heart valve damage.
See also: 5 ways to get creative with employee benefits
There have been a few bright spots in treating obesity prior to this new class of drugs. “Ketogenic” diets with very low carbohydrates are associated with sustained weight loss, although some find this diet hard to maintain. Bariatric surgery leads to an average of 30% weight loss after the first year, although there is some weight gain over subsequent years. Historically, many employers did not cover this, and few promoted it. As a result, only a tiny minority of those who met clinical criteria had bariatric surgery.
What are GLP-1 drugs?
This brings us to this relatively new class of medications, GLP-1 (Glucagon-Like Peptide) agonists, which have been used for over 18 years to treat type 2 diabetes. These drugs reduce appetite and create a feeling of fullness, so people eat less. GLP-1 drugs have been associated with improved blood sugar control and decreased weight. While indicated for type 2 diabetes, these drugs have increasingly been used for weight loss. All but one currently available product is given by self-injection, and side effects often include initial nausea and gastrointestinal upset, which usually resolves over a few weeks. These drugs have a good long-term safety profile when used for treatment of people with diabetes, although they have been associated with rare cases of inflammation of the pancreas and a potential increase in the risk of a rare type of thyroid cancer.
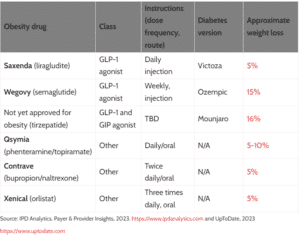
There are two GLP-1 agonists currently marketed for obesity: liraglutide (Saxenda) and semaglutide (Wegovy); a third, tirzepatide, is expected to be approved later this year. There are also multiple additional similar drugs in various stages of clinical trials, several of which will be available in pill form.
These drugs have gained rapid public acclaim. Social media influencers have championed off-label use of the diabetic versions of these medications for weight loss, and these drugs were even mentioned in the opening monologue at this year’s Oscars. Multiple telemedicine companies offer virtual consultations to those seeking prescriptions for these drugs for weight loss.
These drugs have also been endorsed by relevant medical societies. The American Gastroenterologic Association recommends prescribing anti-obesity drugs for those with a Body Mass Index (BMI) of 30 or more, or a BMI of 27 or more if the patient has diabetes or other metabolic conditions This is consistent with labeling approved by the Food and Drug Administration. These criteria make over 40% of adults eligible for treatment, although those with severe kidney disease or who are pregnant or contemplating pregnancy may not be appropriate for this class of medication.
Confronting the cost of anti-obesity drugs
The challenge of the GLP-1 drugs is the cost.
GLP-1 drugs are among the top-cost drugs for employers, and costs of anti-obesity drugs in employer-sponsored health insurance increased by 3.5 times in the first two months of 2023 compared to all of 2022, according to unpublished WTW data.
Net costs (plan and member combined) for each person on Wegovy, after estimated rebates and discounts, is around $9,000 a year. If half of those eligible sought GLP-1 prescriptions, pharmacy cost could increase by over $70 per member per month across the entire population, even assuming some denials and some who would not refill the medications. This is especially unwelcome news to employers facing the highest premium increases in over a decade this year!
Related: Why is Congress watching these 2 drivers of rising healthcare costs?
Obesity is associated with higher medical costs, so widespread use of effective anti-obesity drugs could reduce some future medical expenses. However, the Institute for Clinical and Economic Review (ICER) calculated that these drugs are absolutely not cost-saving. ICER estimates that use of these drugs will cost over $200,000 per quality-adjusted life year, meaning that the cost will far exceed medical savings. These anti-obesity drugs, like most medical care, offer better lives but do not provide cost savings, even over years or decades.
Most employers now provide coverage for bariatric surgery, and the cost of surgery averages about $30,000, although this can vary widely. For employers with high employee turnover, covering GLP-1 medications might be less expensive than covering bariatric surgery. We expect that the availability of this class of medicines will make fewer members seek bariatric surgery.
All employers should keep their eyes on these medications when they are preparing budgets for the coming years. Increased use of these drugs could lower some future healthcare costs, and decrease costs due to absenteeism, productivity loss and mental health spending. Access to these medications could also improve employee recruitment and retention. However, they ultimately will not be cost-saving in the medical budget even at dramatically discounted prices.
The cost of treatment could decrease with multiple new entrants, as happened with hepatitis C antiviral drugs. However, availability of new and improved medications paradoxically raised the prices of existing drugs in some classes of drugs.
Commonly prescribed anti-obesity medications
Considering the options with anti-obesity drugs
Employers have options regarding how or whether to cover these medications. All options include tradeoffs, and different approaches could be more appropriate for different companies. Of note, pharmacy benefit managers might not agree to options that could decrease rebates.
Option 1: Exclude coverage for these medications.
Employers that choose not to cover anti-obesity drugs will have lower drug costs and be able to better restrain increases in member premiums. However, some of their members will seek off-label prescriptions for the versions of these medications approved for diabetes treatment. Higher-wage and more highly educated members are more likely to obtain drugs this way, which could widen inequalities. Employers could find they are at a disadvantage in recruitment and retention if competitors offer coverage.
Option 2: Cover these medications but with restrictions.
Those with severe obesity gain the most from anti-obesity drugs, so some employers could choose a higher BMI to be eligible for coverage. This would lower the cost of medication, and a higher portion of those who were treated would realize medical savings. Some members with BMIs below the threshold might seek off-label diabetes medications.
Some employers may cover these medications but put in place strict rules requiring previous medically supervised diets and a trial of less-expensive anti-obesity drugs before approval. Employees and clinicians dislike prior authorization requirements, and in some instances, this will delay prescriptions, as opposed to preventing them altogether.
Currently, a formulary restriction is difficult because semaglutide is far more effective and convenient than liraglutide. However, a restricted formulary will be more practical once tirzepatide is approved since, like semaglutide, this drug is a weekly injection and associated with 14% or greater weight loss. An employer restricting the formulary to just one of these medications could potentially gain lower acquisition prices.
Option 3: Permissive coverage: Provide coverage for these medications whenever a physician states they are medically necessary with minimal review.
Employers could opt to provide coverage for these medications much as they cover other prescribed medications. Total drug costs will likely be high; members will likely be satisfied, and the company might gain a competitive advantage in hiring.
*
The approval of this new class of weight loss medications is a major advance in medical care, although their currently high costs represent a challenge to employer-sponsored health plans. Companies should be aware of the potential cost implications and should carefully assess benefit design and weigh deploying programs to address potential increases in drug spending.
The following authors contributed to this article:
Chantell Reagan Sell, PharmD is a director and National Pharmacy Practice Clinical Lead at WTW.
Dorothy Wilkes, PharmD is a director in WTW’s Pharmacy Practice organization.
Dennis Barrette, MBA is a director in the Pharmacy Community at WTW.